F-12-114 Clinical Narrative Pathways
🎯 Purpose:
This process identifies the steps required for a PointCare user to add appropriate clinical narrative pathways to print to the 485. These pathways differ from standard pathways as they do not have a POC Goal requirement and do not have associated subsequent visit interventions and goals. The intent of these pathways are to document the primary focus of care, brief clinical summary at time of recert, and functional assessment findings on the 485/POC. Clinician will complete a concise clinical summary that supports the primary focus of care, medical necessity for home health services and recommendations for services.
Jump to:
Documentation Expectations- Clinical Narratives
🔄 Process:
- Select Pathways:

- The Clinical Summary is separated into three pathways to allow for additional documentation:
- Primary Focus of Care OR Recertification Summary
- Functional Assessment Findings
NOTE: There is a character limit of the order text. On a SOC/RCT, if the clinical summary is saved as “incomplete” because future edits are indicated after the completion of the assessment, the edits will need to occur within the Locator 21 Orders (refer to step #10).
- Select the appropriate pathways. Use Recertification Summary during a Recertification Visit. Use Primary Focus of Care Summary at all other time points.

- Ensure the treatment code is selected:

- Each pathway includes a template. Update the order text to reflect the narrative summary. Each required field includes an (*) indicating that it must be completed before saving.
- The Primary Focus of Care Summary should be used to document the Primary Focus of Care and brief narrative to send to the physician.
- There is a character limit within these fields.
- Information entered here should be relevant to the POC, support the POC and needing to go to the provider.
- Additional assessment detail and teaching can be documented within the assessment or a narrative note can be added at the end of the document.

- The Functional Assessment Findings pathway should be used to include documentation to support functional limitations addressed in the OASIS scoring and clinical assessment.
- Refer to F-13-902 Functional Assessment Documentation for additional guidance for documentation to support OASIS answers.

- During the Recertification Visit, select the Recertification Summary instead of the Primary Focus of Care Summary to document a brief summary of the past 60 days and the plan for ongoing services:

- Select Save to save your pathway selection:

-
Once pathways have been selected, the clinician must create the POC. Within the POC Development section, the clinician will have the opportunity to make additional edits to the order (summary) text:
a. Select POC Development:

b. Select Locator 21 Orders:
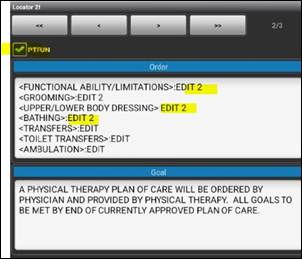
c. Confirm the treatment code is selected and edit text within the Order:
d. Save:




- Clinicians may go back into Pathways to add additional problem statements once they have made the edits in the POC/Locator 21:
-
Select additional pathway to add and edit:
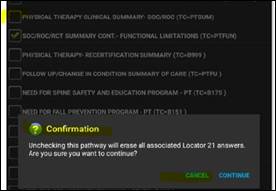
b. If original pathway is UNCHECKED, clinician will get a pop up informing them that all associated Locator 21 (pathway text/orders) will be erased. If they do not want this to happen, they need to select CANCEL:
-


NOTE: Unchecking the original problem statements will remove them from the pathway.
- Clinician may add narrative note if additional assessment information or teaching needs to be documented but does not need to be included on the 485.
- From the main visit screen, select Notes:

b. Select Add:

c. Scroll down and select NARRATIVE note type:

d. Narrative note template includes space for additional assessment detail and teaching performed if applicable:

e. Select menu icon and Save:

Documentation Expectations- Clinical Narratives:
Use the pathway template.
- Complete the Summary of Care using the template included within the pathway in HCHB. The template is intended to guide the clinician with what content to include and has been formatted to print appropriately on the Plan of Care (485).
Do not copy and paste from previous templates.
- Do not copy documentation from previous versions or outside templates into the pathway. The pathway prints as a long narrative, so we have structured it in a way that when it prints to the 485, each section is separated and visible. Copying other templates may result in poor formatting when printed on the 485.
Focus on the Primary Focus of Care.
- The Summary of Care should include only information that supports the Primary Focus of Care, the skilled services being provided, the client's clinical progress, the continued need for home health services, and recommendations to the provider.
- Avoid repeating routine assessment findings or information already documented elsewhere in the visit note or at the end in the narrative note.
Document assessment findings in the appropriate location.
- Comprehensive assessment findings, except for functional assessment findings, should be documented within the appropriate sections of the visit note or within the visit narrative—not within the pathway narrative.
- Functional assessment findings should be documented within the designated pathway.
Sending additional information to the provider.
- If the clinician believes the provider should receive a more detailed summary of assessment findings, complete an External Fax Communication Coordination Note. The External Fax Communication serves as provider notification and does not replace documentation within the medical record. Refer to O-12-101 Initiate an External Fax Communication if needed.
Keep the Summary concise.
-
The pathway has a character limit. Include only information necessary to support:
- the Primary Focus of Care,
- the pertinent clinical status updates,
- the continued need for skilled home health services, and recommendations for ongoing treatment.
- Lengthy assessment narratives or duplication of documentation should not be included.
Narrative Examples:
Example- Skilled Nursing: Primary Focus of Care Narrative:
HOME HEALTH CLINICAL SUMMARY
<<<PRIMARY FOCUS OF CARE>>>: CHF EXACERBATION
<SUMMARY OF NEED FOR SKILLED/PARAPROFESSIONAL SERVICES>: SN TO ADDRESS NEW MEDICATIONS AND CHF EDUCATION/TREATMENT PLAN, MONITOR EDEMA, SKIN ASSESSMENT, RESPIRATORY CHANGES. SN TO PROVIDE EDUCATION TO CAREGIVER ON NEW TELEMONITORING DEVICES. HHA TO ASSIST WITH BATHING AND DRESSING.
<RECOMMENDATIONS>: SN 1W5. PT/OT TO EVAL/TREAT. HHA 2X/WK
HOME HEALTH CLINICAL SUMMARY
<<<PRIMARY FOCUS OF CARE>>>: STAGE 3 PRESSURE ULCER, LEFT BUTTOCK
<SUMMARY OF NEED FOR SKILLED/PARAPROFESSIONAL SERVICES>: SN TO PROVIDE ONGOING ASSESSMENT AND MANAGEMENT OF WOUND INCLUDING EDUCATION TO CAREGIVER AND WOUND CARE AS ORDERED BY PROVIDER.
<RECOMMENDATIONS>: SN 2W4
Example- Skilled Nursing: Recertification Summary:
HOME HEALTH 60 DAY PHYSICIAN SUMMARY OF CARE
<BRIEF SUMMARY OF CARE FROM PAST 60 DAYS>: CLIENT RECEIVED SNV FOR WOUND CARE/ASSESSMENT, PT/OT AND HHA SERVICES FOLLOWING HOSPITALIZATION FOR CELLULITIS AND VENOUS STASIS ULCERS.
<JUSTIFY NEED FOR CONTINUED CARE (RECERT) DUE TO>: CLIENT REQUIRES ONGOING SNV TO PERFORM SKILLED WOUND CARE FOR BILATERAL VENOUS STASIS ULCERS.
<<<PRIMARY FOCUS OF CARE>>>: VENOUS INSUFFICIENCY WITH BILATERAL VENOUS STASIS ULCERS
<RECOMMENDATIONS>: SNV 2X/WEEK FOR WOUND CARE. HHA 2X/WEEK FOR BATHING/LOWER BODY DRESSING.
📅 Effective: 7/13/26 | ✅ Approved by: JS